
Actas del Congreso Nacional de
Tecnología Aplicada a Ciencias
de la Salud
Actas del Congreso Nacional de Tecnología Aplicada a Ciencias de la Salud Vol. 2, 2019
Introducción. La hipotermia perioperatoria inadvertida es hoy en día un problema grave en los entornos quirúrgicos. Existen varios métodos para ayudar a mantener la temperatura corporal del paciente, como la insolación pasiva, la resistencia eléctrica, el aire forzado y la circulación de agua. Este trabajo comienza a explorar el uso de la emisión infrarroja de los semiconductores para estos fines.
Metodología. La radiación de un LED infrarrojo comercial utilizado en telecomunicaciones se aplicó a un sensor de temperatura a diferentes distancias de 0 a 7 mm en intervalos de 0,5 mm. La masa del sensor encapsulado se consideró como la masa a calentar. La intensidad de corriente fue constante durante todo el proceso de medición. La duración de la radiación fue de 200 s para cada distancia. Los resultados de temperatura se procesaron manualmente para modelar el efecto de calentamiento frente a la distancia, considerando la masa objetivo que se calentará y el patrón de apertura de radiación del emisor.
Resultados Las muestras en el osciloscopio muestran claramente una capacidad de calentamiento remoto desde el emisor infrarrojo. La elevación de temperatura disminuye con la distancia entre el emisor y el sensor, de manera exponencial. Una breve prueba muestra que la acumulación de dos emisores que irradian sobre un sensor, causa la superposición del efecto de calentamiento. Entre la distancia mínima posible de un paciente quirúrgico y los datos relacionados con el peso de la piel, se estimó una cantidad de emisores para una lámpara de calentamiento hipotética.
Conclusiones. Debido a la cantidad estimada de emisores necesarios, a pesar de la potencia consumida, esta tecnología es viable para incluirla en un sistema de calentamiento remoto quirúrgico para disminuir la transferencia de calor del cuerpo del paciente al medio ambiente.
Palabras clave: Calentamiento quirúrgico, calentamiento de paciente, calentamiento infrarrojo.
Introduction. Inadvertent perioperative hypothermia is nowadays a serious problem in surgical environments. Several methods exist to help maintaining patient body temperature such as passive insolation, electric resistive, forced air and water circulation. This work begins to explore the infrared emission from semiconductors for these purposes.
Methods. The radiation from a commercial infrared LED used in telecommunications, was applied to a temperature sensor at different distances from 0 to 7 mm and intervals of 0.5 mm. The mass of the sensor capsulated was considered as the mass to warm. Current intensity was constant during all measuring process. Radiation duration was 200 s for each distance. Temperature traces were processed manually to model the warming effect versus distance, considering the target mass to be heated and the radiation aperture pattern of the emitter.
Results. Traces from oscilloscope show clearly a capability of remote heating from the IR emitter. Temperature raising diminish with distance between emitter and sensor, in an exponential way. A brief test shows that the accumulation of two emitters irradiating over one sensor, cause the superposition of the heating effect. Among the minimum possible distance from a surgical patient, and data related to the weight of skin, a quantity of emitters for a hypothetical warming lamp was estimated.
Conclusions. Due to the estimated number of emitters needed, in spite of the power consumed, this technology is viable to be included in a surgical remote warming system to diminish the heat transfer from patient core body to the environment.
Keywords: Surgical warmer, patient warming, infrared warming
Human body presents naturally a thermoregulatory system. Hyperthermia leads to vasodilatation, blushing and sweat, while hypothermia leads to vasoconstriction and shivering. These reactions cause a gradual recuperation of the temperature homeostasis and the maintaining of normothermia (1). Anaesthesia impairs the thermoregulatory system. According to studies, hypothermia in patients about to be intervened has a prevalence of more than 50% (2). Strategies to avoid or diminish inadvertent hypothermia can be divided into two categories: active and passive methods (3). Passive methods include blankets, metalized foils and draping. Active methods include forced air devices, electric resistive blankets and water circulating mattresses (4). According to Moola (5), the most effective way to warm a patient between several active and passive options including radiant devices, is forced air warming (6). The typical radiant device for the mentioned purpose is an infrared incandescent lamp. Such lamp reaches a high temperature in the source of radiation, which is undesirable due to the warming of the nearby area. An infrared light emitter diode is a semiconductor designed to produce light of a specific wavelength. This light, when in the infrared spectrum band, is capable to warm a target mass.
The concept under exploration is to warm the most external layer of skin, in order to diminish the heat transfer from the core of the patient (7). It is considered that a large quantity of IR-LEDs is required for this task.
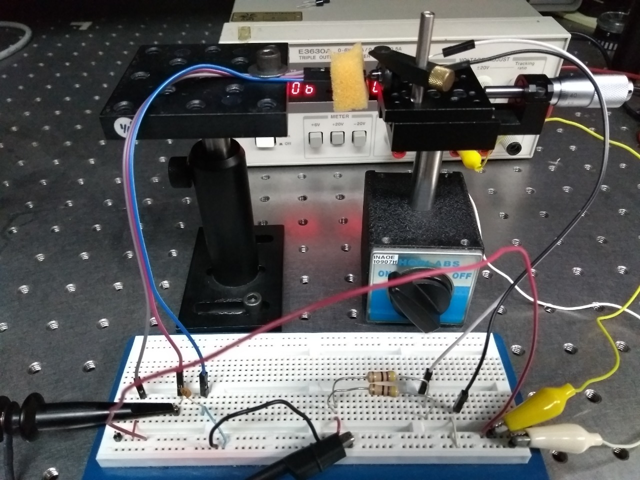
Figure 1. Photo of the experimental array and the electrical circuit used
To characterize the warming capability of the IR333 infrared emitter due to explore the usage of optical semiconductors for biomedical temperature control purposes.
Radiant power of emitters is known from manufacturer datasheets. Even though, the objective is to measure the induction of heat generated by infrared radiation, which is important for the purposes of this work. There is a correlation between irradiation power, distance from and the mass of the target object. Of course, other environment factors and characteristics of the target object do influence on the warming capability, but these are not in the focus of this work.
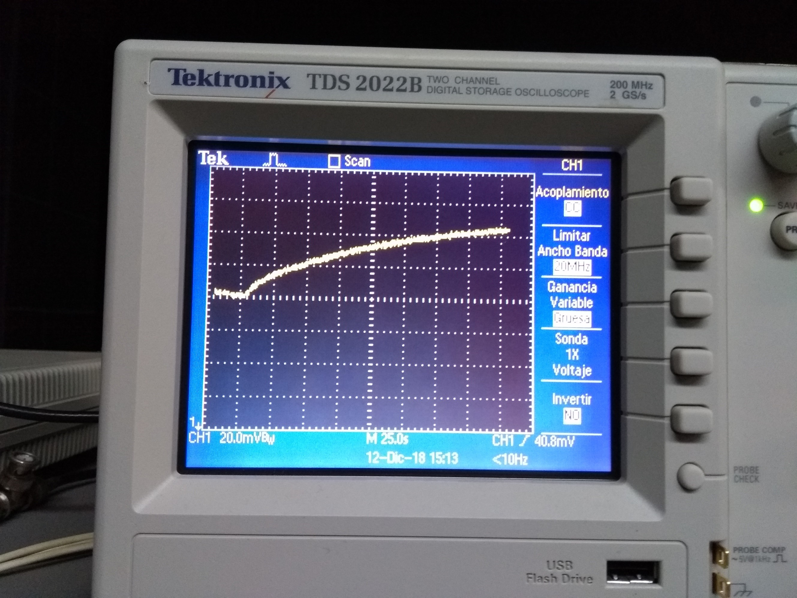
Figure 2. Sample of trace obtained from oscilloscope Tektronix TDS 2022B’s screen
A typical commercial infrared LED for telecommunications and remote controls was selected. It is the IR333 with a radiant power of 85 mW/sr (8), a maximum current of 100 mA, and maximum forward voltage of 1.4 V. For these range of power, the experiment was performed in a mili-scale. Distance was adjusted from 0 to 7 mm from emitter to target. The aperture angle of the beam according to datasheet is 20 degrees. When distance grows, part of radiation is wasted due to an excessive aperture of beam, which is an additional reason for not going beyond 7 mm of distance. Distance was adjusted in 0.5 mm increments for each measure, using a precision screw holder as shown in figure 1. To sense the temperature, a LM35 well known integrated circuit was used with a polystyrene foam side cover to diminish the heat dissipation from the sensor package. This IC brings 10 mV per degree Celsius. A Tektronix TDS 2022B oscilloscope was destined to display the output signal from the sensor. For this low power experiment, a tiny target mass was needed. It was decided to use the temperature sensor package of 0.1897 g as the target mass. The power for the temperature sensor IC must be in the 4 to 20 V range. A voltage of 5 V and an adequate resistor of 25 Ohm was used in order of have a continuous current of 100 mA through the IR-LED, in an array shown in figure 1.
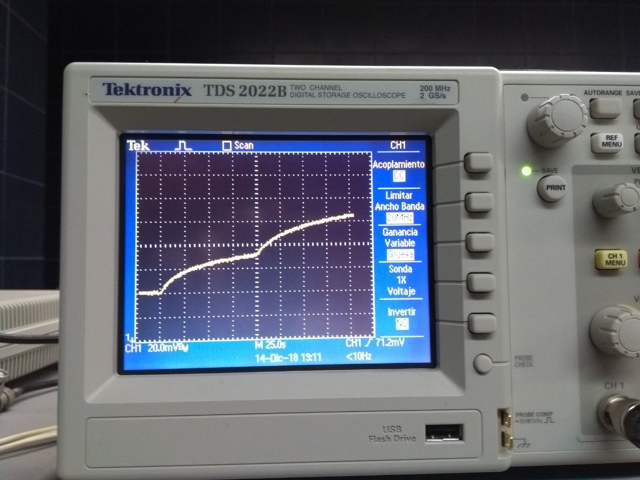
Figure 3. Trace of sensor voltage output, showing the superposition of effects with two emitters irradiating at once.
The sensor was irradiated for 200s as the oscilloscope was registering the voltage fluctuation. Between each of these recordings, a cooling procedure (fresh air blowing) was executed. Each of these 14 traces (from 0 to 7 mm, with distance increments of 0.5 mm) was photographed. A sample of these photographs is shown in figure 2. From the photos, a dataset of temperature increments was manually obtained for exposure times in increments of 10 s this means 20 datasets including an obvious set of cero temperature increments for time cero. The photographed traces showed a notorious noise which leaded the person who took the data to estimate the center of the value in the observation time point in traces.
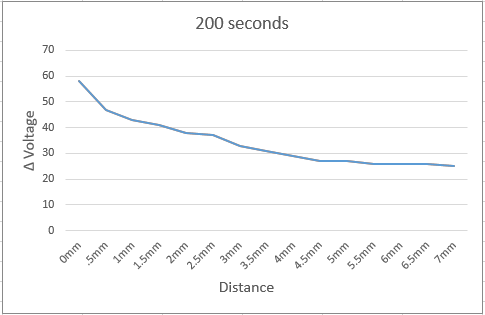
Figure 4. Effects of infrared irradiation depending on distance and exposure time for a mass of 0.1897 g.
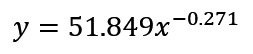
An exponential regression of all the obtained curves was analyzed to obtain the expression relating distance, temperature and time for the tiny mass used in the experiment, shown in formula 1. In order to infer that the accumulation of emitter could have a linear reaction, a simple test was performed in this way: Two emitters were aimed to a unique sensor, from directions separated 60 degrees between them. Irradiation was tested first with one emitter on at a time, and with the two emitters on at once. The obtained trace is shown in figure 3, revealing a clear superposition effect due to the effect of temperature increment with the two emitters at once, being equivalent to the effect of just one emitter, plus the effect of the other.
The curve obtained through data extraction from oscilloscope traces shown in figure 4, describes the effect of infrared irradiation in the target mass temperature, depending on distance and exposure time. The capability of warming the target mass, diminishes with distance and increases with the exposure time. From this data, a second order regression was performed to obtain an analytic model of the increment on temperature through different distances.
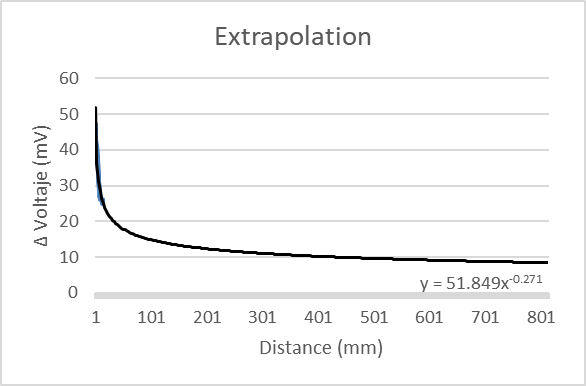
Figure 5. Extrapolating model for the temperature increment effect of infrared irradiation
The graphic obtained with this equation (figure 5) shows the extrapolation of the effect of infrared irradiation at distances quite longer, this is, distances of near 800 mm, expected in operative rooms from instruments and lamps hanged over the operative table, to the patient body. The area of body skin to be heated in a patient can be considered 400 squared cm, which represents the 2.21% of total body surface. The average skin weight in a human body is 3,393 g (9). The concept under this purpose is to warm the skin and slow the transfer of heat from the body´s core to the skin. Thus, the mass of skin to heat is 75 g. Only for estimating purposes, it was considered that an alarming temperature of skin is 34° Celsius. Two degrees Celsius as a temperature increment goal is set. With these values, a quantity of 933 infrared LEDs for a future warming lamp is required.
Almost one thousand LEDs required may seem an excessive quantity, but the experiments for this work were performed over a low power communications LED. Consider that the use of a power LED with 10 times the radiant power of the IR333, the required quantity of LEDs will be near to one hundred. One hundred power LEDs will demand an important intensity of electric current. The management of this current will be an issue of other work. Due to the estimated number of emitters needed, despite of the power consumed, this technology is viable to be included in a surgical remote warming system to diminish the heat transfer from patient core body to the environment.